
Abstract
The present study aims to investigate how dispositional mindfulness affects the mental well-being of cancer patients through the way they perceive stress. A total of 182 moderate and advanced gastrointestinal cancer patients volunteered to complete the Mindful Attention Awareness Scale (MAAS), the Chinese Perceived Stress Scale (CPSS), and the General Health Questionnaire (GHQ). Results showed that perceived stress significantly mediated the relationship between dispositional mindfulness and all dimensions of the mental well-being as captured by the GHQ (i.e. anxiety/depression, social dysfunction, and loss of confidence), and perceived stress was positively correlated with all the dimensions of mental well-being. Results of the Structural Equation Model showed that the model fit the data very well (χ2/df = 1.72,RMSEA = 0.063 (95% CI = 0.014 ~ 0.103), CFI = 0.984, TLI = 0.970, SRMR=0.041). Further analyses showed that dispositional mindfulness predicted all the dimensions of psychological well-being. Specifically, higher levels of dispositional mindfulness predicted reduced subjective perceptions of stress, which in turn predicted lower levels of anxiety/depression, social impairment, and loss of confidence. This study indicated a possible mechanism of intervention focused on improving mindfulness capability. Future work is encouraged to investigate the long-term influence of dispositional mindfulness on perceived stress and psychological well-being in cancer patients with other types of cancer.
Author Contributions
Academic Editor: Shuai Li, Department of Engineering University of Cambridge UK.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Xiaoyan Liu, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Gastrointestinal cancer is an intractable disease with one of the highest incidence and mortality rates in China 1, 2. In the year 2010, 30.77 in every 100 000 Chinese reported having gastric cancer, accounting for 13.08% of the cancer incidence, and the mortality rate for that year was estimated at 21.89 per 100,000 people, accounting for 14.71% of cancer deaths 1. Individuals in moderate to advanced cancer stages experience not only physical, but also psychological distress due to the progression of the disease. Patients with gastrointestinal cancer, in particular, tend to report higher levels of anxiety and depression in comparison to those with other types of cancer 3, and also experience a myriad of negative affect following treatment 4 – both of which may have undesirable consequences on their social functioning and quality of life 5.
Nevertheless, research has shown that the manifestation of mental well-being in cancer patients can differ across individuals 6. One factor which has been increasingly studied as a predictor of psychological well-being improvement and symptom reduction in recent years is dispositional mindfulness. Researchers generally define dispositional mindfulness as an individual ability to obtain a state of awareness that emerges through paying attention to the here and now, in an accepting and nonjudgmental manner 7, 8. In a series of studies, Brown and Ryan 7 showed that dispositional mindfulness was negatively related to psychological symptoms such as anxiety, depression, hostility, and impulsivity. Similar results have been obtained from studies on cancer patients; those with higher levels of dispositional mindfulness showed a lower proclivity for emotional disturbances 6, and reported less sleeping problems 9. In addition, mindfulness-based therapy, which takes dispositional mindfulness as the main target of improvement and development, is of great significance among different psycho-therapies proposed to improve mental health status in the field of psycho-oncology 10.
However, few studies to date have examined the mechanisms underlying the relationship between dispositional mindfulness and psychological symptoms except a small sample study 9 which examined the mediating role of positive reappraisal between dispositional mindfulness and negative emotions in 97 cancer patients. Perceived stress could be one potential mediator of the link between dispositional mindfulness and psychological symptoms. The manifestation of psychological symptoms, such as anxiety and depression, have been found to be associated with poor stress management 11. Tremendous stress can be brought by the cancer diagnosis itself, tedious medical treatment procedures, as well as poor prognosis especially for the patients in moderate to advanced stages. Following the transactional model and conceptualization of stress by Lazarus and Folkman 12, impact of objective stress events is determined by the perception of stressfulness. Among cancer patients, perceived stress has been shown to be a key predictor of anger and depression 13 and negative emotions have been reported up to 12 months later 14.
Grounded on Lazarus’s 12 model, Salmon, Sephton, and Dreeben 15 recently revised the model by integrating the mindfulness component, which proposes that mindfulness can influence every stage of the stress process (e.g., appraisal, coping, emotional outcome, health outcome). Accordingly, mindfulness reduces the degree of stress individual perceived via the promotion of increased present awareness of, and productive responding to, potential stressors (i.e. at the appraisal stage). The improvement of perceived stress acts as a cushion for people against the crucial life stressors and promotes physical and mental health. Findings from previous research are consistent with this proposition 7, 16. Substantial evidence showed negative association between dispositional mindfulness and perceived stress 6, 7, 17, 18, and the effectiveness of mindfulness-based therapy in reducing perceived stress 19, 20. Salmon and colleagues’ 15 model, coupled with the compelling set of findings on the associations between mindfulness, perceived stress, and psychological symptoms, suggest that perceived stress may be one path in which dispositional mindfulness shapes psychological well-being. However, extant evidence to validate the associations between these variables in cancer patients are limited, even more so among gastrointestinal cancer patients at moderate and advanced stages.
The aim of the current study was to examine the relationships between dispositional mindfulness, perceived stress, and manifestation of psychological symptoms using a questionnaire-based study on a sample of Chinese gastrointestinal cancer patients. We hypothesized that perceived stress would mediate the relationship between dispositional mindfulness and psychological symptoms. Specifically, gastrointestinal cancer patients with higher levels of dispositional mindfulness would generally perceive less stress, and consequently would report less psychological symptoms.
Method
Participants
Participants were 200 gastrointestinal cancer patients recruited from a cancer institute in Tianjin. They were required to meet the following criteria: 1) aged 18 years and above; 2) inpatient under treatment; 3) cancer stage II and above; 4) currently not engaged in any psychological intervention or medical treatment on psychiatry. Patients screened in different departments of the tumor. Each patient was accompanied by caregivers, which most were spouses. Most patients come from the city and with no surgery history. Informed consent was obtained from all individual participants included in the study. After removing invalid questionnaires, we were left with 182 participants. Approval for the study was obtained from Ethics Review Committee of Faculty Psychology, Beijing Normal University (reference: 20151103).
Measures
Several measures were edited to assess dispositional mindfulness, perceived stress and mental well-being, such as Mindful Attention Awareness Scale (MAAS), Five Facet Mindfulness Questionaire (FFMQ), Perceived Stress Scale (PSS), The Depression-Anxiety-Stress Scale (DASS), The General Health questionnaire and The satisfaction with life scale (SWLS). All of these scales were validated in Chinese among different samples. However, the physical and mental energy of participants in this study could not afford to complete more items questionnaires. Thus, we conducted three measures with few items but also have high reliability and validity.
Dispositional Mindfulness
The Chinese version 21 of the Mindful Attention Awareness Scale (MAAS) 7 was used to measure dispositional mindfulness. This scale consists of 15 items (e.g., “It seems I’m running on automatic without much awareness of what I’m doing”, “I get so focused on the goal I want to achieve that I lost touch with what I am doing right now to get there.”) rated on a scale of 1 (always) to 6 (not at all). Scores for all items were reverse-coded and summed to form a measure of dispositional mindfulness. Higher scores indicate a higher level of dispositional mindfulness.
Perceived Stress
Perceived stress was captured by the Chinese version 22 of the Perceived Stress Scale (PSS-14) 23. The PSS assesses the degree of perceived stress in the last month using 14 items (e.g., “In the last month, how often have you been upset because of something that happened unexpectedly?”; “In the last month, how often have you felt nervous and stressed?”), rated on a scale of 1 (not at all) to 5 (always). It has two subscales with 7 items in each subscale. The negative subscale is supposed to assess lack of control and negative affective reactions while the positive subscale estimates the capability to cope with stressors. After reverse-coding the scores of 7 items, scores of all items were summed. Higher scores indicated higher levels of perceived stress.
Mental well-being
The General Health questionnaire (GHQ-12) 24 is a widely-used scale which has been shown to have good reliability. It consists of 12 items, rated on a scale of 0 (not at all) to 3 (most of the time), which can be categorized into 3 dimensions – anxiety/depression, social functioning impairment, and loss of confidence 25, 26. Scores of items corresponding to the respective dimensions, and scores of all items were summed to form individual scores for the three subscales and an overall score. Higher scores indicate more severe psychological symptoms.
Procedure
Participants were recruited through advertisements in the consultation room of the hospital. Patients who were interested in the study were given a brief explanation of the study and the assurance of anonymity and confidentiality in their participation. After providing written informed consent, participants completed the questionnaire pack in a quiet room under the instruction of a professional clinician. Upon completion, each patient received monetary compensation for their time and effort. This study was approved by the Ethics Committee of the corresponding author’s university.
Data Analysis
Preliminary analyses involved the use of Pearson’s correlation to examine the associations between the variables we are interested in, and one-way ANOVAs to test the difference on demographic variables. A two-step strategy for mediation analysis was employed following the procedure outlined by Anderson and Gerbing 27. Firstly, we conducted confirmatory factor analysis (CFA) in Mplus 7.1 to test the extent to which the three variables distinct from each other. Then we adopted structural equation modeling (SEM) to identify the fitness of the proposed mediation model. Bootstrap confidence intervals (1000 bootstrap samples) were used to examine the significance of the mediation effect.
In order to reduce inflated measurement errors caused by too many items loading on a single latent construct, parceling strategy which has been widely used for SEM was applied in the MAAS. Highest-loading and lowest-loading items were classified into different parcels successively, and the average score of the items in the same parcel was used. Three parcels had been composited for the MAAS.
Model fit was assessed based on the combinatorial consideration of the following indexes. For an adequate or acceptable model fit, the ratio of chi-square to degree of freedom (χ2/df) should be between 2.0-3.0. The standardized root-mean-square residual (SRMR) and the root-mean-square error of approximation (RMSEA) should ideally be smaller than 0.08. Comparative fit index (CFI) and Good fitness index (GFI) are expected to be >0.90.
Results
Descriptive and Preliminary Analyses
The demographic and clinical information of the current sample were listed in Table 1. It showed that 91.9% of the participants were not religious, 86.4% of participants reported no social stimulation or just general life stress. In terms of the clinical stages, 11 (6%) were at stage II, 92 (50.5%) were at stage III, and 79 (43.4%) were at stage IV. The main types of cancer diagnosed in our sample were stomach cancer, colon cancer, and esophageal cancer.
Table 1. Demographic statistics of participants (N = 182)| Variables | M (SD) or N (%) | Variables | M (SD) or N (%) |
| Age | 56 (11.23) | Marital Status | |
| Gender | Single | 4 (2.2%) | |
| Male | 101 (55.5%) | Married | 173 (95.1%) |
| Female | 81 (44.5%) | Divorced | 2 (1.1%) |
| Education | Widowed | 3 (1.6%) | |
| Primary school | 12 (6.6%) | Household monthly income | |
| Middle / high school | 116 (63.7%) | <2000 RMB (~280 USD) | 55 (30.2%) |
| Bachelor’s degree | 55 (27.5%) | 2,000 - 5,000 RMB | 92 (50.5%) |
| Graduate degree or above | 4 (2.2%) | 5,001 - 10,000 RMB | 27 (14.8%) |
| >10,000 RMB | 8 (4.4%) |
The means, standard deviations, internal reliability coefficients and correlations among variables are presented in Table 2. Dispositional mindfulness was negatively associated with perceived stress and degree of psychological symptoms reported (ps < 0.05). Positive correlations were found between perceived stress and psychological symptoms (ps < 0.01).
Table 2. Means, standard deviations (SD), Cronbach’s alpha coefficients, and correlations of the variables.| 1 | 2 | 3 | 4 | 5 | 6 | |
| 1 CPSS | 1 | |||||
| 2 MAAS | -0.28*** | 1 | ||||
| 3 GHQ -T | 0.68*** | -0.25** | 1 | |||
| 4 GHQ - AD | 0.58*** | -0.23** | 0.80*** | 1 | ||
| 5 GHQ - SD | 0.51*** | -0.18* | 0.78*** | 0.32*** | 1 | |
| 6 GHQ - LC | 0.46*** | -0.17* | 0.73*** | 0.58*** | 0.35*** | 1 |
| M | 36.63 | 63.38 | 11.24 | 5.33 | 4.28 | 1.63 |
| SD | 10.18 | 10.48 | 6.36 | 3.02 | 3.44 | 1,71 |
| Cronbach’s α | 0.79 | 0,81 | 0.82 | 0.78 | 0.74 | 0.69 |
MAAS, Mindfulness Attention Awareness Scale; CPSS, Chinese Perceived Stress Scale;
GHQ -T, total scores of General Health Questionnaire; GHQ –AD, Anxiety/Depression of GHQ;
GHQ –SD, Social dysfunction of GHQ; GHQ –LC, Loss of confidence of GHQ.
Preliminary analyses revealed that age was not significantly related to mental well-being as a whole, as captured by the GHQ total score (p > 0.250). Moreover, results from one-way ANOVAs showed that psychological symptoms did not differ significantly by gender, education level, income level, marital status, and stage of disease. Therefore, all this demographic information was excluded from consequent analyses. The plots of correlations of the variables were presented in Figure 1, Figure 2, Figure 3.
Figure 1.Plot of correlation between MAAS and GHQ
Figure 2.Plot of correlation between MAAS and CPSS
Figure 3.Plot of correlation between CPSS and GHQ
Measurement Model
The measurement model consisted of three interrelated latent variables including dispositional mindfulness, perceived stress, and mental well-being. Dispositional mindfulness was created by three parcels with 5 items in each parcel 28. Mental well-being was created by three indicators which were anxiety/depression, social functioning impairment and loss of confidence. Perceived stress was indicated by two explicit indicators: positive items and negative items. The results of the CFA analysis on the measurement model demonstrated adequately fit to the observed data: χ2/df = 1.72,RMSEA = 0.063 (95% CI = 0.014 ~ 0.103), CFI = 0.984, TLI = 0.970, SRMR=0.041.
To identify the possible common method variance (CMV) resulted from the fact that all the variables were measured by self-reported instruments, Harman’s single-factor test was utilized following Podsakoff ’s 29 method. According to the principle of Harman’s test, CMV exists when the one-factor model fits well or majority of the total variance (e.g. more than 50%) can be explained by one general factor. The one factor model did not have a good fit, with each fitness index far from the standard thresholds (χ2/df = 13.72,RMSEA = 0.264, CFI = 0.626, TLI = 0.476, SRMR=0.156), which indicated that CMV might not have a significant impact on our results.
Structural Model for Mediation
Structural relationship proposed among all the variables were examined (see Figure 4). The results demonstrated that our hypothesized mediating model fit the data in an adequate way, χ2/df = 1.77, RMSEA = 0.065 (95% CI = 0.021 ~ 0.104), CFI = 0.982, TLI = 0.968, SRMR=0.046.
Figure 4.Path coefficients of the model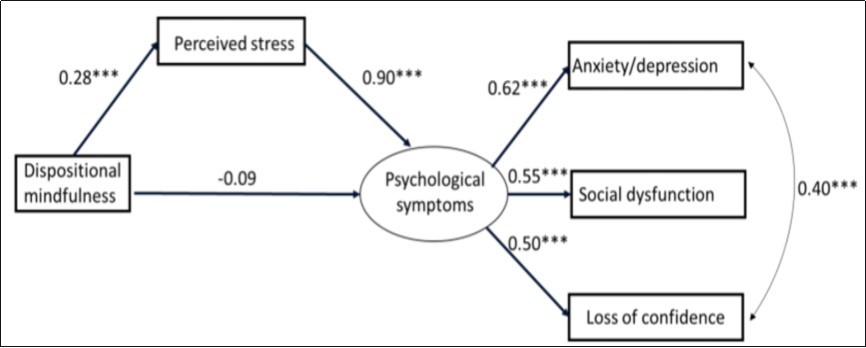
To examine the mediation effect of perceived stress, we compared the full mediation model against the partial mediation model 30. To be specific, the path from dispositional mindfulness to psychological symptoms was constrained to zero in the full mediation model while not constrained in the partial mediation model. The fitness index in each condition was showed in Table 3. It is recommended using CFI difference to conduct model comparisons with the rule of thumb as close to or smaller than 0.05. Since the CFI difference (0.002) in our study was smaller than 0.05, the full mediation model regarding the relation between dispositional mindfulness and psychological symptoms was rejected.
Table 3. The fitness index in each condition| X2/df | RMSEA(95%CI) | CFI | TLI | SRMR | |
| Full-mediation | 1.77 | 0.065[0.021~0.104) | 0.982 | 0.968 | 0.046 |
| Partial mediation | 1.72 | 0.063[0.014~0.103) | 0.984 | 0.970 | 0.041 |
Next, Bootstrap analysis was used to test the significance of the indirect relationship 31. No distributional requirement on the indirect effect based on the bootstrap estimation makes the result of the mediation effect more accurate. From the data set (N=182), using random sampling with replacement, 1000 bootstrap samples were generated. The exclusion of zero in the confidence interval (CI) indicates the significance of the indirect effect. Our results showed the significant indirect effect on psychological symptoms from dispositional mindfulness via perceived stress (Standard indirect effect = -0.255, 95% CI = -0.378 ~ -0.133, zero was not in the 95% CI).
Next, separate analyses were conducted to investigate the role of perceived stress as a mediator of the relationship between dispositional mindfulness and each of the three psychological symptoms - anxiety/depression, social functioning impairment and loss of confidence. As presented in Table 4, the results indicated that perceived stress significantly mediated the associations between dispositional mindfulness and all the three outcomes.
Table 4. Mediation results of perceived stress (subscales of GHQ as dependent variables)| Path | Indirect effect | 95% CI | |
| Upper | Lower | ||
| Dispositional Mindfulness – Perceived stress – Anxiety/Depression | -0.046 | -0.073 | -0.024 |
| Dispositional Mindfulness – Perceived stress – Social functioning impairment | -0.047 | -0.076 | -0.023 |
| Dispositional Mindfulness – Perceived stress – Loss of confidence | -0.021 | -0.033 | -0.011 |
Discussion
The current study examined the relationships between dispositional mindfulness, perceived stress, and psychological symptoms for the first time among gastrointestinal cancer patients in moderate and advanced stages. Our findings are therefore of valuable contribution to existing literature since the majority of past findings have been derived from cancer patient samples with relatively lower mortality rates and functioning impairments 14 (e.g. breast cancer). In line with previous research, the current findings showed that cancer patients with higher dispositional mindfulness reported lower levels of perceived stress 32 and psychological symptoms 6, 9, 18, while perceived stress positively predicted psychological symptoms 13, 14.
More importantly, our findings demonstrated the role of perceived stress as a mediator of the relationship between dispositional mindfulness and psychological health. That is, more mindful gastrointestinal cancer patients tended to perceive lower stress in their day-to-day life within the last months, and this, in turn, contributed to lower experience of psychological symptoms, such as loss of confidence, anxiety, and impairment in social functioning. These findings shed light on one path in which mindfulness can improve psychological wellbeing, thus supporting Salmon and colleagues’ 15 proposition on how mindfulness can influence stress process. The benefits of mindfulness on stress appraisal, as suggested by the negative relationship between mindfulness and perceived stress in the current study, may be attributed to a higher tendency to focus on the present, and to be more accepting, not only of oneself as cancer patient, but also of the experiences related to the disease which may serve as potential stressors 7, 33. Some of these experiences, such as pain and fear of death have been shown to be the most common source of stress for cancer patients 34, 35. Mindfulness, for instance, may help alleviate feelings of pain and other physical discomfort as well as fear of death 36, hence reducing feelings of stress. It would be worthwhile for future studies to examine the role of multiple (serial) mediators in the relationship between mindfulness and psychological health. By obtaining a more sophisticated understanding of the specific ways (e.g., through regulation of pain or negative emotions) that mindfulness can lead to reduced stress and better psychological health, mindfulness-based training interventions can be fine-tuned to focus on the cultivation of skills in specific areas which may be more effective than others.
Nevertheless, the current findings highlight the utility of mindfulness-based training interventions to foster improvement of dispositional mindfulness 19, 20 among cancer patients. Our findings imply that such interventions would not only improve stress management or specifically, the way people appraise stressful experiences related to the disease, but through this, also improve their psychological wellbeing. Following Salmon and colleagues’ 15 model, and empirical evidence from psycho-oncology research 37, such improvements can also have a positive effect on the immune system, or physical health in general – perhaps contributing to prolongation of survival. Caution should be exercised in generalizing our findings to patients with other forms of cancer since the current study concentrated on moderate and advanced gastrointestinal cancer patients, whose survival periods are shorter than other kinds of cancer patients. Due to the cross-sectional design of the present study, we were unable to verify the causality of the mediation model.
Conclusion
The present data showed that the perceived stress mediated the relationship between dispositional mindfulness and psychological symptoms in gastrointestinal cancer patients. Our study should be considered as an initial attempt to explore the relationships between these variables in patients with gastrointestinal cancer, as most previous findings have come from cancer patients with relatively low mortality and impaired function. Future research should consider the longitudinal effects of dispositional mindfulness on perceived stress and psychological health, and should include other measures that can better inform current findings, such as the level of pain experienced and the fear of death.
Acknowledgments
This study was supported from the Project of Philosophy and Social Science Research in Colleges and Universities in Jiangsu Province entitled Intervention effect and mechanism of localized mindfulness training on psychological trauma of adolescents after the Yancheng Tornado (No. 2017SJB0218).
We gratefully thank the researchers of the Center of Mindfulness Research.
References
- 1.Chen W, Zheng R, Zhang S, Zhao P, Zeng H et al. (2014) Report of cancer incidence and mortality in China. , Annals of Translational Medicine 2(7), 61-86.
- 2.Hu Y. (2003) Follow-up Study on Anxiety, Depression and Quality of Life of Chinese Patients Newly Diagnosed with Gastrointestinal Cancers. , CHINESE MENTAL HEALTH JOURNAL 17(12), 810-812.
- 3.Gonen G, S U Kaymak, E S Cankurtaran, E H Karslioglu, Ozalp E et al. (2012) The factors contributing to death anxiety in cancer patients. , Journal of Psychosocial Oncology 30(3), 347-358.
- 4.Olsson U, Bergbom I, Bosaeus I. (2002) Patients’ experiences of the recovery period 3 months after gastrointestinal cancer surgery. , European Journal of Cancer Care 11(1), 51-60.
- 5.Xu C. (2005) A discussion about effect of psychological factor and social factor on the prevention and treatment of gastrointestinal tumor. , CHINESE JOURNAL OF CLINICAL PSYCHOLOGY 13(2), 250-252.
- 6.L E Carlson, K W Brown. (2005) Validation of the Mindful Attention Awareness Scale in a cancer population. , Journal of Psychosomatic Research 58(1), 29-33.
- 7.Brown K W, Ryan R M. (2003) The benefits of being present: mindfulness and its role in psychological well-being. , Journal of Personality and Social Psychology 84(4), 822-848.
- 8.Wang F, Huang Y-X. (2011) Psychological and neural mechanisms of mindfulness. , Advances in Psychological Science 19(11), 1635-1644.
- 9.E L Garland, Thielking P, E A Thomas, Coombs M, White S et al.Linking dispositional mindfulness and positive psychological processes in cancer survivorship: a multivariate path analytic test of the mindfulness‐to‐meaning theory. , Psycho‐oncology 26(5), 686-692.
- 10.Piet J, Würtzen H, Zachariae R. (2012) The effect of mindfulness-based therapy on symptoms of anxiety and depression in adult cancer patients and survivors: A systematic review and meta-analysis. , Journal of Consulting and Clinical Psychology 80(6), 1007-1020.
- 11.Vollrath M, Torgersen S. (2000) Personality types and coping. , Personality and Individual Differences 29(2), 367-378.
- 12.R S Lazarus, Folkman S. (1984) Coping and adaptation. The Handbook of Behavioral Medicine 282-325.
- 13.P S Lee, J N Sohn, Y M Lee, E Y Park, J S Park. (2005) A correlational study among perceived stress, anger expression, and depression in cancer patients. , Journal of Korean Academy of Nursing 35(1), 195-205.
- 14.D M Golden-Kreutz, L M Thornton, Gregorio W-D, G M Frierson, H S Jim et al. (2005) Traumatic stress, perceived global stress, and life events: prospectively predicting quality of life in breast cancer patients. , Health Psychology 24(3), 288-296.
- 15.P G Salmon, S E, S J Dreeben. (2011) Mindfulness‐Based Stress Reduction. Acceptance and mindfulness in cognitive behavior therapy: understanding and applying the new therapies. 132-163.
- 16.J D Creswell, B M Way, N I Eisenberger, M D Lieberman. (2007) Neural correlates of dispositional mindfulness during affect labeling. , Psychosomatic Medicine 69(6), 560-565.
- 17.Bao X, Xue S, Kong F. (2015) Dispositional mindfulness and perceived stress: The role of emotional intelligence. , Personality and Individual Differences 78, 48-52.
- 18.S N Garland, Campbell T, Samuels C, L E Carlson. (2013) Dispositional mindfulness, insomnia, sleep quality and dysfunctional sleep beliefs in post-treatment cancer patients. Personality and Individual Differences. 55(3), 306-311.
- 19.Bränström R, Kvillemo P, J T Moskowitz. (2012) A randomized study of the effects of mindfulness training on psychological well-being and symptoms of stress in patients treated for cancer at 6-month follow-up. , International Journal of Behavioral Medicine 19(4), 535-542.
- 20.Speca M, L E Carlson, Goodey E, Angen M. (2000) A randomized, wait-list controlled clinical trial: the effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. , Psychosomatic Medicine 62(5), 613-622.
- 21.Deng Y-Q, Li S, Tang Y-Y, Zhu L-H, Ryan R et al. (2012) Psychometric properties of the Chinese translation of the mindful attention awareness scale (MAAS). , Mindfulness 3(1), 10-14.
- 22.Yang T, Huang H. (2003) An epidemiological study on stress among urban residents in social transition period. Zhonghua liu xing bing xue za zhi= Zhonghua liuxingbingxue zazhi. 24(9), 760-764.
- 23.Cohen S, Kamarck T, Mermelstein R. (1983) A global measure of perceived stress. , Journal of Health and Social Behavior 385-396.
- 24.Goldberg D. (1978) Manual of the general health questionnaire: Nfer Nelson. , Windsor, Bershire, UK
- 25.Gao F, Luo N, Thumboo J, Fones C, Li S-C et al. (2004) Does the 12-item General Health Questionnaire contain multiple factors and do we need them? Health and Quality of Life Outcomes. 2(1), 63-70.
- 26.Li Y, Li Y. (2015) The factor structure of the 12-item General Health Questionnaire: The multi-group analyses. , Chinese Psychological Exploration 35(4), 355-359.
- 27.J C Anderson, D W Gerbing. (1988) Structural equation modeling in practice: A review and recommended two-step approach. , Psychological Bulletin 103(3), 411-423.
- 29.P M, S B MacKenzie, Lee J-Y, N P Podsakoff. (2003) Common method biases in behavioral research: A critical review of the literature and recommended remedies. , Journal of Applied Psychology 88(5), 879-903.
- 30.Li S, Karatzoglou A, Gentile C. (2016) Collaborative filtering bandits. Paper presented at the. Proceedings of the 39th International ACM SIGIR conference on Research and Development in Information Retrieval .
- 31.A F Hayes, N J Rockwood. (2017) Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. , Behaviour Research and Therapy 98, 39-57.
- 32.Tamagawa R, Giese‐Davis J, Speca M, Doll R, Stephen J et al. (2013) Trait mindfulness, repression, suppression, and self‐reported mood and stress symptoms among women with breast cancer. , Journal of Clinical Psychology 69(3), 264-277.
- 33.Kabat‐Zinn J. (2003) Mindfulness‐based interventions in context: past, present, and future. Clinical psychology: Science and Practice 10(2), 144-156.
- 34.M S Ali, Osmany M, Khan W, Mishra D. (2014) Fear of death, depression and coping among cancer patients. , Indian Journal of Health and Wellbeing 5(6), 681-686.
- 35.P A Glare, P S Davies, Finlay E, Gulati A, Lemanne D et al. (2014) Pain in cancer survivors. , Journal of Clinical Oncology 32(16), 1739-1747.
Cited by (1)
- 1.Nowakowska‐Domagała Katarzyna, Podlecka Marlena, Sadowski Karol, Pietras Tadeusz, Mokros Łukasz, 2023, The relationship between chronotype, dispositional mindfulness and suicidal ideation among medical students: mediating role of anxiety, insomnia and social dysfunction, Journal of Sleep Research, 32(4), 10.1111/jsr.13823