
Abstract
Background
Prevalence of coronary artery disease is between 7-13 percent in urban and 2-7 % in rural India1. The alarm in rise in the prevalence of coronary risk factors like diabetes, hypertension, dyslipidemia, smoking, central obesity and physical inactivity2. The correlation between these risk factors and the severity of coronary atherosclerosis, assessed by angiography which may be either single or multivessel is less consistent with studies reporting conflicting results 3,4. Therefore our study aims to understand the proper correlation between risk factors and severity of coronary artery disease in an Indian population
Methods
This study was conducted in the department of cardiology, NIMS hospital Hyderabad which receives patients from the urban as well as rural areas of Telangana. the patients admitted in the department of cardiology, NIMS hospital Hyderabad that presented with acute coronary syndromes and diagnosed to have coronary artery disease (single vessel/multivessel disease) on coronary angiography taken for study. Sample Size is 150
Results
Among the 150 subjects, males were 111(74%) and females were 39(26%). Mean age of the study population is 55.2 ± 11.4. Among SVD group 73.65% were males &26.3% were females. Among MVD group 76.2% were males & 23.7% were females. Mean age for SVD was 53±14.4 years, while mean age foe MVD was 58.6±14.5 years. For ACS mean age of presentation for females is 60.7±11.4 and for males mean age of presentation is 55.1±12.6. MVD (57.2%) were more common among smokers than SVD. In <45 years age group SVD (69.2%) were more common than MVD (30.8%). In 45- 70 years age group and >70 years age group MVD were more common than SVD with 69.6% and 66.6% respectively, which is statistically significant. MVD (60%) were more common among hypertensives than SVD. Among non-hypertensives MVD (41.8%) was less common than SVD (58.2%) MVD was common among all age groups, which is statistically signicant. Among STEMI group SVD (58.3%) was more common than MVD (41.7%). Among NSTEMI group MVD (62%) was more common than SVD (38%).Correlation between groups was statistically significant. Among SVD study group, LVEF was commonly between 30-45% & very few with LVEF <30% MVD was associated with more severe LV dysfunction as compared to SVD in acute MI. The difference in ejection fraction between the two groups was statistically significant P value=0.0002. In hospital MACE Among SVD there was 1 MI (due to stent thrombosis) who had to TVR (primary PCI) & rest were asymptomatic and discharged in normal state MVD there were in hospital deaths (due to refractory cardiogenic shock) rest were asymptomatic and were discharged in normal state. This difference between the two groups was statistically insignificant.
Conclusion
Multivessel disease in ACS were seen more commonly among elderly as compared to young subjects where single vessel disease were more common. Females especially elderly more commonly have multivessel disease. Mean age for multivessel disease was higher than single vessel disease. Among <45 years age group, SVD was more prevalent among smokers, obese and physically active. Multi vessel disease is more prevalent among patients with risk factors like diabetes, hypertension, dyslipidemia and physically inactive. Subjects with family history of premature CAD presented early and correlated well with prevalence of SVD.NSTEMI presented more with multi vessel disease. In echocardiographic wall motion analysis, a depressed regional segment of infarcted area with remote hyperkinesis predicted SVD where as remote area hypokinesis predicts more multivessel disease. In hospital outcomes were seen among multi vessel disease as compared to single vessel disease although not statistically significant.
Author Contributions
Copyright © 2022 Rama Kumari Nuthalapati, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Prevalence of coronary artery disease is between 7-13 percent in urban and 2-7 % in rural India1. The alarm in rise in the prevalence of coronary risk factors like diabetes, hypertension, dyslipidemia, smoking, central obesity and physical inactivity2. The correlation between these risk factors and the severity of coronary atherosclerosis, assessed by angiography which may be either single or multivessel is less consistent with studies reporting conflicting results3,4. Therefore our study aims to understand the proper correlation between risk factors and severity of coronary artery disease in an Indian population. Once this initial evaluation is performed, laboratory blood tests, an echocardiography, and then coronary angiography may be necessary to obtain further diagnostic insight. A ECG is a simple, non invasive and important bedside diagnostic tool in the diagnosis of ACS. Echocardiography remains the most frequently used and usually the initial imaging test to evaluate all cardiovascular diseases related to structural, functional or hemodynamic abnormality of heart or great vessels. Invasive coronary angiography (CAG), the gold standard for diagnosis of CAD in patients presenting with ACS, defines therapeutic options and determines prognosis. This study has been done to compare the clinical profile (age, sex, major risk factors, comorbidities, outcomes) ECG and echocardiographic findings between single and multi-vessel disease in patients presenting with ACS. In order to understand the different modes of presentation of single vessel and multivessel disease, its association and correlation with various risk factors, co morbidities and prognosis in patients presenting with ACS. This knowledge of different profiles in acute coronary syndromes will help us to understand and plan both preventive and curative treatment strategy in future. Hence we did this study to compare the clinical profile (age, sex, various risk factors), electrocardiographic profile, echocardiographic profile (global LVEF, wall motion score index (WMSI), and diastolic function (E/e1 ratio) between single vessel and multi vessel disease in patients with acute coronary syndromes (ACS), To evaluate and compare in hospital outcome between single vessel and multivessel disease.
Materials and Methods
This study was conducted in the department of cardiology, NIMS hospital Hyderabad which receives patients from the urban as well as rural areas of Telangana
Study Population: the patients admitted in the department of cardiology, NIMS hospital Hyderabad who presented with acute coronary syndromes and diagnosed to have coronary artery disease (single vessel/multivessel disease) on coronary angiography taken for study. We compared the age, sex, ECG, ECHO profiles in both patients with SVD and MVD.
Sample Size: 150
Study Period: MAY 2019 –DECEMBER 2020
Study method: a prospective, observational and longitudinal study
Inclusion Criteria
Consenting patients
All patients of any age or either sex admitted with acute coronary syndromes Patients diagnosed as acute myocardial infarction found to have CAD either single or multi vessel disease on coronary angiography between MAY 2019-DECEMBER 2020.
Exclusion Criteria
Previously diagnosed acute coronary syndromes patients
Previous PCI or CABG
Patients with valvular heart disease
Patients with dilated cardiomyopathy
Patients with hypertrophic obstructive cardiomyopathy
Patients with pericardial disease
Patients with myocarditis
Patients on cardiovascular devices
Statistical Analysis
Statistical analysis was done using SPSS software version 26.0. continuous variables is presented as mean and median is data is unevenly distributed. categorical variables are expressed as frequencies and percentages. P values were calculated and P values less than 0.05 was considered as statistically significant.
Results
Among the 150 subjects, males were 111(74%) and females were 39(26%). Mean age of the study population is 55.2 ± 11.4. Among SVD group 73.65% were males &26.3% were females. Among MVD group 76.2% were males & 23.7% were females. Mean age for SVD was 53±14.4 years, while mean age foe MVD was 58.6±14.5 years. For ACS mean age of presentation for females is 60.7±11.4 and for males mean age of presentation is 55.1±12.6.
MVD (57.2%) were more common among smokers than SVD. In <45 years age group SVD (69.2%) were more common than MVD (30.8%). In 45- 70 years age group and >70 years age group MVD were more common than SVD with 69.6% and 66.6% respectively, which is statistically significant.
MVD (60%) were more common among hypertensives than SVD. Among non-hypertensives MVD (41.8%) was less common than SVD (58.2%) MVD was common among all age groups, which is statistically significant.
Among diabetes subjects MVD (62.7%) was more common than SVD (37.2). In <45 years age group no difference was seen between SVD or MVD. Among >45 years age group MVD was seen more commonly than SVD. The difference between two groups is statistically significant.
Among normal BMI group SVD (66.7%) were more common than MVD (33.3%). Among over weight group, MVD (65.7) were more common than SVD (34.2%).Among obese group, MVD (66.6%) were more common than SVD (33.3%).Association was statistically significant between two groups. Among subjects with positive family h/o premature CAD, SVD (66.6%) was more common than MVD (33.4%).Among subjects with negative family h/o premature CAD, MVD (54.1%) was relatively more than SVD (45.9%)Therefore, patients with family history of premature CAD tend to present early & have more SVD.
Among STEMI group SVD (58.3%) was more common than MVD (41.7%).Among NSTEMI group MVD (62%) was more common than SVD (38%).Correlation between groups was statistically significant. Among SVD study group, LVEF was commonly between 30-45% & very few with LVEF <30% MVD was associated with more severe LV dysfunction as compared to SVD in acute MI. (Figure 3) The difference in ejection fraction between the two groups was statistically significant P value=0.0002, as shown in table 1.
Table 1. MACE between patients with Single vessel disease and Multivessel disease| Variables | Death | MI | Stroke | Angina | TVR | Asymptomatic | |
| Mace in Hospital | SVD | 0 | 1.60% | 0 | 0 | 1.60% | 98.30% |
| MVD | 3.20% | 0 | 0 | 0 | 0 | 96.70% | |
In hospital MACE Among SVD there was 1 MI (due to stent thrombosis) who had to TVR (primary PCI) & rest were asymptomatic and discharged in normal state MVD there were in hospital deaths (due to refractory cardiogenic shock) rest were asymptomatic and were discharged in normal state. This difference between the two groups was statistically insignificant, as shown in (Figure 1, Figure 2).
Figure 1.Graph showing age and sex distribution among single/multivessel disease
Figure 2.Graph showing correlation of STEMI/MSTEMI with Single/multivessel disease in acute MI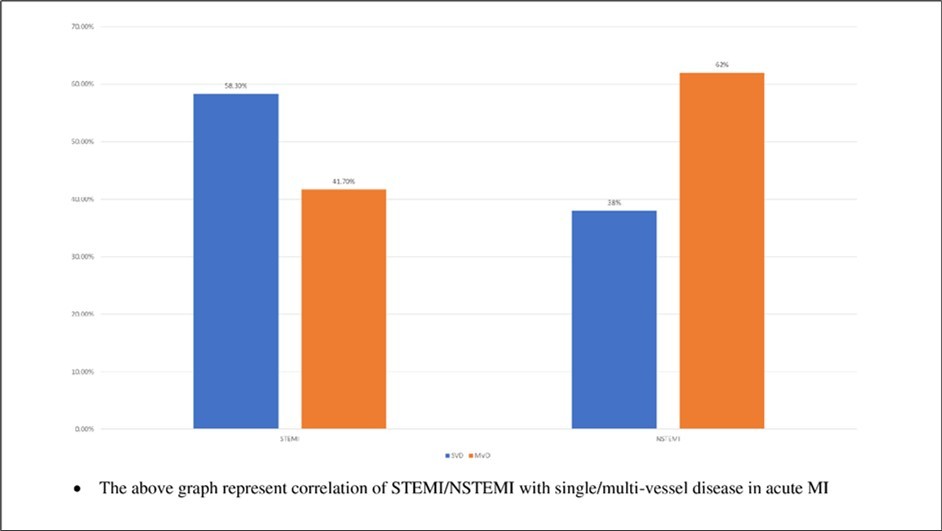
Figure 3.Graph showing corelation of LV ejection fraction in single/multivessel disease
Discussion
Series of subjects presenting to cardiology ICCU at NIMS hospital between May 2019 to December 2020 who were diagnosed to have ACS were subjected to coronary angiography, on basis of which was categorised in to single and multivessel disease. Various clinical parameters, ECG changes, Echo features and outcome parameters were noted and compared among single and multivessel disease with acute coronary syndromes. In study by Sharma R et al,5 mean age group were 54.71± 19.9yrs, males were 79.5%& females were 20.5%. In study by Navin K et al, mean age group were 56.1±10.5 yrs., males were 83.3% with mean age of 55.7±10.6 & females were 16.7% with mean age of 58.25±9.69 years. In our study smokers were found to be associated more among males with MVD (57.2%) than SVD (42.85%) is similar to study done by Zanda Parsa et al6 where MVD were 54% than SVD (31%) which explains well that smoking promotes atherosclerosis. On other hand our study found among young smokers the prevalence of SVD was more (69.2%) compared to MVD (30.8%), In our study 61% subjects were hypertensive with MVD (60%) and SVD (40%). In all age groups MVD were more common than SVD. Study by Bduansyah Tengku et al7 published in journal of hypertension 2015 has 58% hypertensive subjects and among them 18%were SVD, 70% were MVD & 12% Were normal coronaries. The analysis of our subjects in respect to dyslipidemia showed MVD predominance in angiography (MVD vs SVD-9% vs 41%). Study by Rafaela Andrade et al also showed the predominance of MVD among dyslipidemics more so with elevated triglyceride/HDL ratio. An increased accumulation of fat in the intrabdominal cavity, termed as visceral adiposity is highly correlated with an adverse coronary risk profile. The study done in our centre showed prevalence of multivessel disease in subjects with BMI >25kg/m2 (66.6%) compared to SVD (33%) but study by Rubinshtein R et al8found no significant association of higher BMI with MVD. Our study showed that PCI/CABG is being performed with a high procedural success rate and good long term clinical outcome. It is not associated with an increased rate of stent thrombosis or late major clinical adverse events. The angiographic success rate was 98% in our study.
The multi vessel disease was associated with risk factors like diabetes, hypertension, dyslipidemia and physically inactivity and patients with a family history of premature coronary artery disease presented with SVD. The patients with MVD may be linked to the inactivation of critical anti-aging genes such as Sirtuin 1. Sirtuin 1 has been shown to be defective in diabetes, cardiovascular disease, dyslipidemia and exercise has been shown to activate Sirtuin 1. In developing countries chronic diseases has been shown to be linked to the inactivation of Sirtuin 1 with relevance to ACS. 9, 10, 11, 12
In the present study, we found that MVD and stent implantation were relatively more associated with only one death. Studies by Chow et al. and De Waha et al both reported that the severity of CAD not only predicted all cause mortality but also were high risk factors for adverse clinical outcomes. The higher morbidity and mortality are seen in ST segment elevation MI patients with multivessel CAD.
Limitations
In our study sample size is very small and this prevented us from obtaining sufficient data among SVD and MVD to study the significant differences. This study was a single centre study where patients were randomly selected. However, the study is unique in the sense that no patient with prior MI was included in this study. A large sample size with study population from various backgrounds will help to determine the effect of ACS risk factors.
Conclusion
Multivessel disease in ACS were seen more commonly among elderly as compared to young subjects where single vessel disease were more common. Females especially elderly more commonly have multivessel disease. Mean age for multivessel disease was higher than single vessel disease. Among <45 years age group, SVD was more prevalent among smokers, obese and physically active. Multi vessel disease is more prevalent among patients with risk factors like diabetes, hypertension, dyslipidemia and physically inactive. Subjects with family history of premature CAD presented early and correlated well with prevalence of SVD.NSTEMI presented more with multi vessel disease. In echocardiographic wall motion analysis, a depressed regional segment of infarcted area with remote hyperkinesis predicted SVD where as remote area hypokinesis predicts more multivessel disease. In hospital outcomes were seen among multi vessel disease as compared to single vessel disease although not statistically significant.
References
- 1.Sekhri T, Kanwar R S Wilfred, Chugh R, Chhillar P, Aggarwal M et al. (2014) Prevalence of risk factors for coronary artery disease in an urban Indian population. 4(12), 5346-5347.
- 2.Gus I, R A, Kato S, Bastos J, Medina C et al. (2014) Variations in the Prevalence of Risk Factors for Coronary Artery Disease in Rio Grande do Sul-Brazil: A Comparative Analysis between2002and2014. Arquivos brasileiros decardiologia. 105(6), 573-582.
- 3.Uddin S N, Malik F, Bari M A, Siddiqui N I, Khan G K et al. (2005) Angiographic severity and extent of coronary artery disease in patients with type 2 diabetes mellitus Mymensingh Med. , J 14(1), 32-39.
- 4.Zand Parsa AF, Ziai H, Haghighi L. (2012) The impact of cardiovascular risk factors on the site and extent of coronary artery disease. , Cardiovasc J Afr 23(4), 197-206.
- 5.Sharma R, Bhairappa S, S R Prasad, Manjunath C N. (2014) Clinical characteristics, angiographic profile and in hospital mortality in acute coronary syndrome patients in south indian population. Heart India. 2, 65-9.
- 6.Zand Parsa AF, Ziai H, Haghighi L. (2012) The impact of cardiovascular risk factors on the site and extent of coronary artery disease. , Cardiovasc J Afr 23(4), 197-199.
- 7.Budiansyah Tengku, Wibowo Rd Robin H, Syafitri Rosa, Tantono. (2015) Angiographic Profile between Hypertensive and Non Hypertensive Patients in Hasan Sadikin Hospital. , Journal of Hypertension 33(1), 31.
- 8.Rubinshtein R, Halon D A, Jaffe R, Shahla J, Lewis B S. (2006) Relation between obesity and severity of coronary artery disease in patients undergoing coronary angiography. , Am 97(9), 1277-1280.
- 9. (2016) Anti-Aging Genes Improve Appetite Regulation and Reverse Cell Senescence and Apoptosis in Global Populations. Advances in Aging Research 5, 9-26.
- 10. (2017) Single Gene Inactivation with Implications to Diabetes and Multiple Organ Dysfunction Syndrome. , J Clin Epigenet 3(3), 24.